CT COULD PROVE TO BE THE BEST METHOD FOR STUDYING CARDIOVASCULAR ABNORMALITIES
Statistics show that coronary heart disease is rising every year and has reached pandemic proportions. Although it has had a tendency to decrease in developed countries, owing to improved diagnostics and prevention, in developing and transitional countries it is steadily rising.
Every year, CT (computed tomography) is improving. As of now, CT is considered the “gold standard” for diagnosing coronary artery stenosis and other coronary anomalies. There have also been many studies proving efficacy of CT for planning coronary artery bypass surgery, performing electrophysiology studies and investigations of the pulmonary veins.
MRI on the other hand, has proven valuable in diagnosing a range of conditions including cardiomyopathies, cardiac anatomical anomalies (congenital and acquired), functional abnormalities, cardiac and pericardial masses and diseases of the aorta and great vessels.
The inherent advantages of using CT are reduction of motion artifacts, enhanced spatial resolution (coronary arteries are normally 25 mm in diameter), improved contrast resolution (for investigating, for example, soft plaques), reduced scan times (less than one breathhold) and reduced radiation exposure (compared to coronary angiography).
"With the evolution of CT machines, we are able to cover the whole heart in one or two rotations, which is really amazing, and decrease the contrast and radiation dose greatly, while increasing the spatial resolution and image quality," said Dr. Ahmed Samir Ibrahim, an associate professor of radiology at Ain Shams University in Cairo.
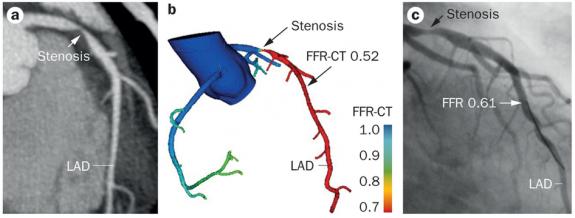
Fractional flow reserve (FFR) is a wirebased procedure that measures blood pressure and flow in the coronary arteries. FFR is done during coronary catheterization and includes a guide wire with a transducer tip to measure temperature, pressure and flow to evaluate lesion severity.
With the addition of FFR, coronary CT angiography (CCTA) can improve patient care and outcome. During conventional angiography physicians may be tempted to stent any blockage of the coronary arteries (oculostenotic reflex). Studies show that this approach is not evidencebased and that only functional measurements (FFR) can show that blood flow is not significantly affected and that the patient does not require stenting and can be treated with medical therapy.
Qualitative and quantitative data from CCTA has been proven to be as or more informative than invasive coronary angiography and intravascular ultrasound. But what sets CCTA apart from these other procedures is the simplicity and effectiveness with which it allows the study of preclinical stages of atherosclerosis. This facilitates improved risk assessment and prognosis based on the extent of coronary atherosclerosis and specific characteristics of plaque.
24.04.2015